The British government on Monday (14 June) eased blood donation rules for gay, bisexual and queer men – yet activists warn harmful restrictions remain.
Blood donation rules in England, Scotland and Wales have long screened out donors if they are a man who has had oral or anal sex with another man.
This is because male donors were asked to disclose whether they have had sex with another man during checks.
But coming into effect on World Blood Donor Day and following recommendations from a health committee, British blood services will now assess donor eligibility on a person-by-person basis instead of applying a blanket restriction.
So, rather than just men, all people regardless of gender and sexuality will be asked the same questions on recent sexual activity, if any.
This means anyone who has had the same sexual partner for the last three months will be eligible, allowing more LGBT+ folk than ever before to donate blood, platelets and plasma.
It’s a long-sought for shift in policy quickly hailed as “historic” by top LGBT+ advocates, but sexual health groups warned that the blood donation process is still riddled by “barriers”.
“Patient safety is at the heart of everything we do,” said the blood service’s chief nurse for blood donation Ella Poppitt.
“This change is about switching around how we assess the risk of exposure to a sexual infection, so it is more tailored to the individual.
“We screen all donations for evidence of significant infections, which goes hand-in-hand with donor selection to maintain the safety of blood sent to hospitals.”
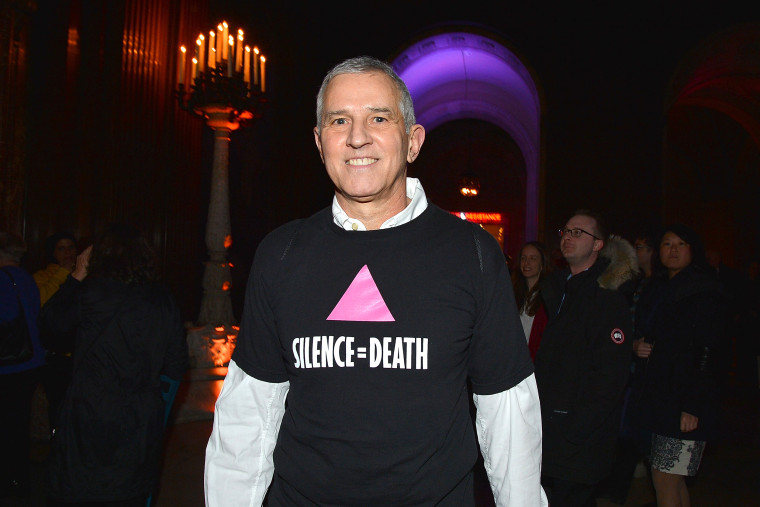
For Eric Sawyer, the 40th anniversary of the first scientific report that described AIDS as a new disease brings up “a dichotomy of feelings.”
When Sawyer, who was living in New York, first began exhibiting symptoms of HIV in 1981, he said he was urged by his friend, the late activist and playwright Larry Kramer, to begin seeing “a doctor who’s also gay, who is seeing patients with this disease.”
That same year, across the country, a young physician named Michael Gottlieb and his colleagues at UCLA wrote in an official Centers for Disease Control and Prevention report about patients diagnosed with a lung infection common in what would come to be called AIDS.
“In the period October 1980-May 1981, 5 young men, all active homosexuals, were treated for biopsy-confirmed Pneumocystis carinii pneumonia at 3 different hospitals in Los Angeles, California. Two of the patients died,” the report, published on June 5, 1981, in the CDC’s Morbidity and Mortality Weekly Report, stated.
Eric Sawyer attends the “Love & Resistance: Stonewall 50” event at New York Public Library on Feb. 14, 2019.Patrick McMullan / Getty Images file
Sawyer, now 67, recalled being told by a doctor, at just 32, to put his affairs in order.
“In addition to being elated that I have survived for 40 years with this illness, I also have a certain degree of survivor’s guilt,” Sawyer, a founding member of AIDS activist group ACT UP New York, told NBC News. “Why me? Why did I deserve to survive when so many of my friends and a couple of my boyfriends died really horrible, ugly deaths at very young ages?”
Four decades after the CDC published the now-historic report, long-term survivors like Sawyer, as well as HIV/AIDS activists and doctors, are reflecting on their experiences on the front lines of the crisis and warning of the inequities that have allowed it — which has killed an estimated 34.7 million people globally since the epidemic began, according to UNAIDS — to persist.
“AIDS in the United States is not over, and especially it’s not over in the Global South or around the world,” said Jawanza James Williams, the director of organizing at VOCAL-NY, a nonprofit that helps low-income people impacted by HIV and AIDS. “There’s a sort of tendency to talk in the past tense, as if HIV and AIDS, as an epidemic, has been ended in the States, and it erases the realities and the experiences of Black people, of brown people, or poor people, people that are uninsured, and it really misses the mark.”
People of color are disproportionately impacted by HIV, according to the CDC. Of new HIV diagnoses in the U.S. in 2018, Black Americans accounted for 42 percent and Latinos accounted for 27 percent.
‘Something clicked’
Gottlieb’s encounters with the patients he would end up documenting in his June 5, 1981, CDC report started with one gay man “whose immune system was kind of totaled by something.” Then, within a month, there were three patients just like the first, he recalled. They were all between the ages of 29 and 36.
“Something clicked. There’s something going on that is very unusual and needs to be reported to someone,” said Gottlieb, now an HIV and internal medicine specialist at Los Angeles-based APLA Health, a network of Federally Qualified Health Centers that serve LGBTQ people and people impacted by HIV.
While the CDC uses the date of the report to mark the start of the HIV/AIDS epidemic, “that’s not factually correct,” Gottlieb said.
Prior to 1981, evidence suggests that Robert Rayford, a 15 year-old boy, died in St. Louis in 1969 from a condition later identified as AIDS.
Later in the 1970s, there were accounts of individuals becoming sick with parasites or what was then called “Gay bowel disease,” “and it probably was HIV, but we didn’t know it,” Dr. Howard Grossman, a primary care physician specializing in HIV treatment and prevention, told NBC News.
For activists and survivors, the history of the HIV crisis transcends a linear timeline that can forget the nuance of human experience, according to Ted Kerr, a writer and organizer whose work focuses on HIV/AIDS.
“My No. 1 fear is that people will think that HIV started 40 years ago, and what that does is it suggests that HIV begins when the United States government says it begins,” Kerr said. “Actually for me, it begins when someone’s journey with HIV starts. So, the history of HIV starts tomorrow for somebody when they get their HIV diagnosis. HIV started in 1969 for the Rayford family in St. Louis when Robert died, and, of course, that also includes the June 5 article from the CDC.”
‘New homosexual disorder’
As a gay man in medical school in New York in the early 1980s, Grossman, now the medical director of Midway Specialty Care Center in Wilton Manors, Florida, said the first stories he heard of people getting what would eventually be known as AIDS were imbued with “judgment” about drug use and promiscuity.
In an article from May 1982, The New York Times referred to the disease as a “new homosexual disorder.” A month later, in NBC News’ first report on the mysterious illness, “Nightly News” anchor Tom Brokaw reported that a new study found “the lifestyles of some male homosexuals has triggered an epidemic of a rare form of cancer.”
When Grossman attended a packed meeting convened by Larry Kramer and the newly formed Gay Men’s Health Crisis in 1983, “that was when people realized something really bad was going on,” he said.
As a medical resident in a Brooklyn hospital that same year — when much of the public still thought this mysterious illness primarily affected gay men — Grossman saw intravenous drug users, people of Caribbean descent and women who, in retrospect, he believes were exhibiting symptoms of AIDS.
Less than a decade later, Ivy Kwan Arce, a long-term survivor of AIDS and an ACT UP member, said she encountered disbelief when she asked her doctor for an HIV test after seeing an ACT UP poster that said, “Women don’t get AIDS. … They just die from it,” with fine print recommending that women with multiple sexual partners or who are drug users get tested.
After Kwan tested positive, she had to retest because the attitude was that “maybe the test was wrong.” She ended up at an ACT UP meeting at The Lesbian, Gay, Bisexual & Transgender Community Center.
At the time, the CDC’s definition of AIDS excluded medical conditions experienced by women who were later known to have the disease, causing the government to undercount the number of women who had died due to AIDS-related complications. Kwan participated in activism that pushed the government to expand the definition of AIDS to include specific conditions for women, alongside Katrina Haslip, an HIV/AIDS activist and fellow ACT UP member who died in 1992 from complications of AIDS, according to a New York Times obituary.
Kwan had been working as a graphic designer, but when her workplace found out she was HIV positive, she said they announced her diagnosis to her co-workers, forbade her from using the bathroom and asked for a calendar of her menstrual cycle before she was eventually fired.
More than 30 years after her diagnosis, Kwan said, the narrative for women living with HIV/AIDS “has not changed a whole lot.”
Jawanza James Williams, who was diagnosed with HIV at 23, said various communities that were responding to the crisis early on have been erased from AIDS history.
“It suggests that somehow Black folks, brown folks, women, trans people weren’t on from day one, responding with love to this crisis and still are,” he said.
Looking back to move forward
When Williams was diagnosed with HIV in 2013, he said he thought about the more than 30 years that had lapsed since President Ronald Reagan first publicly said the word “AIDS” in 1985. By the end of that year, the U.S. had more than 16,000 reported cases of the then-fatal illness.
For Williams, his diagnosis was also a moment of realization.
“It wasn’t some unique sexual behavior,” Williams, now 31, said of why he contracted the virus. Instead, he said he realized it was because of systemic reasons — such as race, location and class — and his close proximity to communities that are disproportionately impacted by HIV/AIDS.
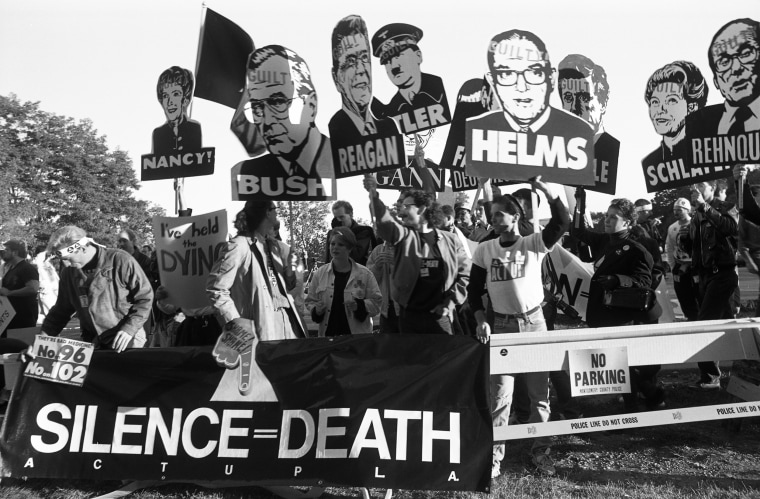
Members of AIDS activist group ACT UP hold up signs of George W. Bush, Ronald Reagan, Nancy Reagan, Jesse Helms and others with the word “Guilty” stamped on their foreheads, along with a banner stating “Silence Equals Death” at a protest at the FDA headquarters on Oct. 11, 1988, in Rockville, Md.Catherine McGann / Getty Images file
While there is currently an effective HIV-prevention drug available for those at risk of contracting HIV, and a pill with few side effects that can treat those who are already living with the virus, Sawyer does not want the public to overlook the hundreds of thousands of people around the globe who contract HIV and die from AIDS-related complications annually. In 2020, an estimated 1.5 million people became newly infected with HIV, and 690,000 people died from AIDS-related illnesses, according to global statistics from UNAIDS.
“That’s far too many people dying and far too many people getting infected with what is a fatal disease if you don’t get access to the latest medical interventions and the latest medications,” said Sawyer, a co-founder of Housing Works, an organization working to end the dual crisis of homelessness and AIDS.
For Sawyer, the 40th anniversary of the historic June 5, 1981, report is a moment to recognize the lessons that “AIDS should have taught us.”
“It’s time we start caring about the health of everyone on this planet,” he said.
May 17 is the International Day Against Homophobia, Transphobia, Biphobia and Intersexphobia (IDAHOBIT). Along with Pride month, it is a time when the global spotlight shines on LGBTIQ equality. Every year we need that spotlight, because, while progress has been inspiring in recent decades, the levels of exclusion, discrimination, harassment and violence LGBTIQ communities around the world continue to face every day are harrowing. Over the last year and a half they have only been amplified by the pandemic.
In recent weeks we hear more and more about increasing COVID-19 vaccine access in the USA, in the U.K., and elsewhere. We hear about restrictions easing, and about life going back to a semblance of normalcy. What we hear less about are the countries where vaccines are a long way from being available, and the people being left behind from recovery efforts. Among them, LGBTIQ people.
So on this IDAHOBIT, I want the spotlight to shine on that.
Vulnerable communities are always more deeply affected in times of crisis. In the U.S., Black and Latinx people continue to become infected and die from COVID-19 at much higher ratesthan white people. The United Nations highlights that millions more women worldwide have lost jobs in the pandemic and have had to bear more of the burden of caring for children and elderly family members.
For LGBTIQ people, the marginalization that we experience on a day-to-day basis was amplified during the pandemic. Due to overrepresentation in informal sector jobs caused by employment discrimination, LGBTIQ people experienced a devastation of livelihoods. Loss of homes and an inability to leave resulted in higher rates of domestic violence. We’ve experienced amplified challenges accessing health care, and increasing mental health issues due to separation from communities. Moreover, LGBTIQ people, as in other crises, have been blamed and scapegoated for the COVID-19 pandemic, further amplifying already prevalent levels of LGBTIQ-phobia around the world.
Compounding that even further is the fact that humanitarian responses often exclude LGBTIQ people by using narrow definitions of family, binary definitions of gender, unsafe locations, or biased staff for emergency interventions.
In April 2020, OutRight launched a COVID emergency fund to support LGBTIQ communities around the world. Reflecting the ongoing crisis the LGBTIQ community is facing, the latest call for applications, launched last month, received 1,500 applications from 111 countries, totaling $26 million in need. Applications highlighted a deepening crisis as LGBTIQ people continue to be out of jobs, continue to have to live with abusive family members, and face challenges accessing life-saving care for HIV, gender affirming treatment, or, indeed COVID-19. One applicant highlighted a dramatic loss of funding as a result of which they are on the brink of shutting several community centers providing crucial services to the community. Another highlights an exponential growth in calls for help to their hotline, with most callers asking support for shelter and food, as well as psychological support due to abuse and violence in the home.
At the same time, while vaccines have become widely available across North America and Europe, the same is not true for the majority of the world. This vaccine tracker shows less than one dose administered per 100 people across Africa, one to two in parts of the Middle East and Southeast Asia. The picture looks more hopeful in Latin America, with over 80 people out of a 100 having received a dose in Chile, and just over 20 in Brazil.
What does this mean? That most people in the world have not reached the end of the pandemic. And, as the Global South has more of the world’s population and more of the world’s laws criminalizing same-sex relations, the majority of LGBTIQ people in the world will continue to be in a crisis within a crisis, feeling amplified effects. Experience also shows that when recovery efforts do take on more speed, LGBTIQ people will not be among the first to feel the effects — they will be among the last.
Days like IDAHOBIT are a time for reflection. A pandemic hurts every one of us. It cannot be overcome unless everyone is included in the recovery effort. These days can also be a time to honor interdependence, and to recognize that we are stronger together. At this moment in the pandemic, LGBTIQ people, other marginalized communities, and people across the Global South are being forgotten. Until everyone is included normalcy will not return, the pandemic will continue to evolve, and we will continue to be at risk.
Maria Sjödinm is Deputy Executive Director, OutRight Action International.
Patrick O’Connell, a venerable AIDS activist who sought to smash stigma with awareness campaigns such as the iconic red ribbon, has died.
O’Connell passed away aged 67 of AIDS-related causes, his brother Barry confirmed to The New York Times.
Living with HIV for 40 years, he spent much of his life fronting campaigns to better educate the public about what it means to live with HIV/AIDS.
The son of a wire lather and secretary, O’Connell was born 12 April, 1953, in post-war New York City.
For much of the 1980s, O’Conell’s life was filled with rented black funeral suits and friends fearful of what was then a dooming diagnosis. By the end of the decade, AIDS had become the leading cause of death for men aged between 25 and 44.
In 1991, O’Connell formed Visual AIDS, a collective of artists and advocates who used a borrowed art gallery space to design exhibitions that forced the public to reckon that the disease.
We had no choice,” he said in a 2003 interview with the BBC. “We had to do something with our professional lives.
“The East Village art scene felt like it was disappearing overnight because of AIDS. All our colleagues around the country were dying.”
No wonder. The White House was, at the time, almost indifferent to the virus’ rampage across the US and treated it more as a punchline than a public health emergency.
That’s when O’Connell had an idea: a small way to encourage the world to reckon with the disease that was destroying so much of the LGBT+ community – a red ribbon.
That same year he launched the Ribbon Project and with it, an unwavering and defiant symbol of AIDS activism.
To O’Connell, the colour red was as rousing as it was morose. It symbolised, he told the BBC, blood. It is “the colour of passion” and is “vibrant and attention-getting”.
The yellow ribbons from the Gulf War were still all around,” he told The New York Timesin 1992. “We noticed that they could mean anything from ‘I care about young people who have gone overseas’ to ‘I support Bush.’
“We wanted that kind of leeway, too, something that could mean ‘I hate this government’ or just ‘I care about people with AIDS’.”
In the two weeks before the 1991 Tony Awards, the 15 artists involved in Visual AIDS oversaw the making of thousands of grosgrain ribbons which were delivered to the Minskoff Theatre.
As the awards were beamed into homes across America, host Jeremy Irons walked on – and he was wearing a red ribbon.
Soon enough, whether it be pinned on a dress worn by Elizabeth Taylor or printed on United States Postal Service-issued stamps, the red ribbon was everywhere.
O’Connell’s death comes after that of Larry Kramer, the ACT UP agitator who fought against policy-makers to take the disease seriously, and Nita Pippins, who was something of a mother figure to countless AIDS patients.
“It is hard to be prideful of something that was generated by such frustration and sorrow,” O’Connell reflected of his decades-long work in AIDS activism to the BBC.
“I would give anything, I would give back all this attention if I hadn’t lived through these decades of AIDS.
“All the people who died so young, these talented people. Now I know only one person alive from my 20s.”
HIV-positive Americans are at a high risk for intimate partner violence, with one in four (26.3 per cent) having experienced it at least once, new data has shown.
The findings from the Centers for Disease Control and Prevention (CDC), published in the American Journal of Preventive Medicine, used data from the Medical Monitoring Project, “a surveillance system designed to learn more about the experiences and needs of people who are living with HIV”.
The study showed that not only are HIV-positive people in the US at higher risk of physical abuse at the hands of their intimate partners, but that “intimate partner violence is associated with adverse health consequences among people with diagnosed HIV”.
It also showed that 4.4 per cent had experienced intimate partner violence within the last 12 months.
Researchers from the CDC’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention and the National Center for Injury Prevention and Control found that people with HIV who had recently suffered intimate partner violence were “more likely to engage in behaviours associated with elevated HIV transmission risk”, like intravenous drug use or high-risk sex, and “have unmet needs for supportive services”.
They were also “less likely to be engaged in routine HIV care but were more likely to seek emergency care services and have poor HIV clinical outcomes”.
The lifetime prevalence of intimate partner violence among people with HIV varied depending on gender and sexual orientation. The highest risk group was HIV-positive bisexual women, of whom more than half had experienced physical abuse from a partner.
Those who had been homeless within the past 12 months were also at a higher risk (37.6 per cent) than those who had not (25.2 per cent).
Researchers said it was “important” that HIV-positive Americans are screened for intimate partner violence at initial HIV tests, as well as during routine appointments.
This, they said, “may help address issues of missed medical visits, poor [antiretroviral treatment] adherence, and difficulty attaining and maintaining viral suppression”.
They added: “When intimate partner violence is identified, supportive services should be offered.
“With these additional supportive services, the safety and health of people with HIV may be improved.”
President Biden, unveiling on Friday his initial budget request to Congress in the first year of his administration, called for ramping up funds to beat the HIV/AIDS epidemic in the United States, signaling he’d continue the PrEP-centric initiative that began in the previous administration.
In the preliminary budget request for fiscal year 2022, known in Washington parlance as the “skinny budget” in anticipation of broader request at a later time, Biden seeks an increase of $267 million for Ending the HIV Epidemic, building on the more than $400 million Congress has appropriated for the program since 2019.
As it was launched in the Trump administration, the initiative sought a 90 percent decrease in new incidents of HIV infections across the United States by 2030, although Biden campaigned on beating that goal by five years and ending the domestic HIV epidemic by 2025.
Carl Schmid, executive director of the HIV+Hepatitis Policy Institute, hailed in a statement the proposed increased funds for the initiative, but said it falls short of the amount advocates in the fight against HIV/AIDS were seeking.
“While it falls short of what the community has requested, if this funding is realized it will continue the momentum already created and make further progress in ending HIV in the U.S. Efforts to end HIV will help eradicate an infectious disease that we have been battling for the last 40 years and help correct racial and health inequities in our nation,” Schmid said.
Counterintuitively, Trump had sought more funds to beat HIV/AIDS in his final year in office than Biden has in his first year in office. Last year, President Trump’s budget called for an increase of $412 million for the second year of the initiative for a total of $716 million while Congress settled on an increase of approximately $137 million.
Biden seeks increased funds for HIV/AIDS at a time when advocates in the fight against HIV were at a crossroads at the start of a new administration. Questions had persisted about whether or not the Biden administration would continue the initiative, which was the brainchild of health officials in the Trump administration.
With the inauguration of President Joe Biden, I hope we may now see the kind of leadership on LGBTQ issues we need. As a gay African-American man living with HIV, I have lived through two pandemics. Under both HIV/AIDS and COVID-19, LGBTQ people have had to shoulder the burden of discrimination while fighting to survive. I hope that 2021 is the year that changes.
I was diagnosed with HIV in 1984, in the early years of the epidemic. I lost many friends in the years that followed. So many of us in that time never expected to live a full life ourselves. After watching our friends die, it became hard to imagine that we’d ever make it to our 40th birthday — let alone retirement. The discrimination we experienced and the looming threat of the virus made it difficult to build careers and save for the golden years we never thought we’d see. I’ve lost jobs due to discrimination myself, and the stress of it nearly killed me. That’s why today, I help advocate for LGBTQ elders and folks on social security.
I have seen every stage of the HIV/AIDS crisis, from the pandemic, to its aftermath, to the present day. I know how much work it takes to survive and thrive in the face of this virus. As the administrator of a group home for folks recovering from HIV-related hospital stays, a member of the local HIV Planning Council, and a care outreach specialist for a community clinic, I’ve seen the kind of discrimination people still face. I once worked with a pregnant woman who was turned away from a local hospital for being HIV-positive. Because our clinic existed, she got the care she needed and her baby was born healthy.
In recent years, advances in prevention and access to testing and treatment have led to encouraging declines in new diagnoses. But stigma and anti-LGBTQ bias continue to have consequential effects on testing decisions. Time and again, I have spoken with clients who choose to hide their condition or status to avoid ostracization and discrimination. According to a recent research report by the Williams Institute at the University of California, Los Angeles, 44 percent of Black LGBTQ adults have either never been tested, tested when they felt at risk, or once every two years or less. It’s an alarming statistic that falls far too short from CDC recommendation for testing frequency for HIV, which is at least once a year or more frequently.
Despite these challenges, it’s possible to live a full and healthy life with HIV/AIDS. As Americans, we should be able to participate in all aspects of daily life with dignity and respect, and without fear of discrimination. If we wholeheartedly want to end the HIV epidemic in the United States, we must seize the moral high ground and ensure LGBTQ Americans are provided with equal rights, better access to care, and increased secure housing. Federal nondiscrimination legislation will help us get there.
Although it’s important to celebrate how far we’ve come, right now, 50 percent of LGBTQ people live in the 29 states that lack comprehensive statewide laws explicitly prohibiting discrimination against LGBTQ people, including here in my home state of Georgia. And in the midst of a pandemic and the accompanying economic crisis, it’s inhumane that millions of us can still be denied housing or medical care just because of who we are or who we love. Situations like these enable the spread of HIV.
Our nation is going through a profound change, but our values of treating others as we would want to be treated remains the same. The Equality Act would ensure that all LGBTQ Americans can live, work, and access public spaces and medical care free from discrimination, no matter what state we call home. It’s the right thing to do — which is why this type of legislation has broad and deep support across lines of political party, demographics, and geography. Public support is at an all-time high, with 83 percent of Americans saying they favor LGBTQ nondiscrimination protections, including 68 percent of Republicans and a majority in every state in the country.
After all, equality is not a Democratic or Republican value, it’s an American value. It’s also the smart thing to do as we work to end the HIV epidemic in America.
Nathan Townsend is a 66-year-old Black gay man living and thriving with HIV for 36 years. He devotes his time and efforts helping to promote health equity and equal access to care for his community.
Virginia lawmakers have approved legislation modernizing laws around HIV exposure.
Passed after two versions of the bill were reconciled, the legislationwould repeal the felony criminal ban on blood, tissue or organ donation by people with HIV and other sexually transmitted infections; make HIV-testing for people convicted of certain crimes, including prostitution and drug charges, optional rather than mandatory; and strike down a statute making failure to disclose HIV-positive status before sex a Class 1 misdemeanor punishable by up to 12 months jail time.
Intentional transmission of HIV, or “infected sexual battery,” would remain a felony in Virginia, rather than a misdemeanor, as proponents had hoped, but the new legislation would require proof of actual infection, rather than just exposure.
The bill now heads to Gov. Ralph Northam, a Democrat, who has until March 31 to sign the measure into law. While Northam has not specifically said he would sign the bill, he has previously signed pro-LGBTQ bills, including one requiring schools to create policies related to the treatment of trans students and a ban on so-called conversion therapy.
Virginia state Sen. Jennifer McClellan, a Democrat, who introduced the bill with fellow Democrat and state Sen. Mamie Locke, said HIV criminalization laws are an ineffective public health tool that disproportionately affect the LGBTQ community and people of color.
“They target and stigmatize people who are HIV positive, even though being HIV positive is itself not a threat to public safety.” McClellan told NBC News. “It makes people less likely to disclose or get tested.”
There’s also the question of determining someone’s intention to expose a partner.
“It’s so hard to prove,” McClellan said. “There have been instances where you’ve had a bad breakup and someone will swear out a warrant, saying ‘You tried to infect me,’ or use it as a threat.”
According to the Centers for Disease Control and Prevention, 37 states have laws criminalizing intentional transmission of HIV. Many were enacted after Congress approved the federal Ryan White Comprehensive AIDS Resources Emergency (CARE) Act in 1990. That landmark legislation provided millions of dollars in health care and support services for people with HIV. But to qualify, states had to enact laws allowing for the prosecution of anyone “who knowingly and intentionally exposes a nonconsenting individual to HIV.”
In the intervening decades, understanding and treatment of HIV have grown exponentially. But leading health organizations, including the American Medical Association, the World Health Organization and the CDC itself, say the laws have not caught up with advances in science.
According to the CDC, many HIV laws criminalize behavior that cannot transmit the virus — including spitting or biting — and can be applied whether or not there is actual transmission. They also don’t account for advances in HIV medication, which can keep an individual’s viral load undetectable, presenting zero risk of transmission.
Before Saturday, only six states had modernized their criminalization laws since 2014: California, Colorado, Iowa, Michigan, North Carolina and Washington, according to the advocacy group Equality Virginia. Just one, Texas, has repealed its laws.
While Virginia’s law has rarely been enforced, between 2019 and 2020 three people in the state were convicted of felony infected sexual battery and misdemeanor sexual battery, according to the Roanoke Times.
McClellan’s bill, which made infected sexual battery a misdemeanor, passed the Senate 21-17 earlier this month. But a version keeping the felony charge intact cleared the House of Delegates 56-44 Friday. In negotiations to reconcile the two bills, the House version prevailed.
Some lawmakers were concerned the language in McClellan’s bill would allow someone to intentionally transmit HIV without fear of prosecution.
“I find it stunning that we would want to eliminate the felony for what is potentially fatal, deadly conduct,” state Sen. Mark D. Obenshain, a Republican, told The Washington Post.
McClellan argues there are other laws about intentionally infecting someone with a disease, including those prohibiting “malicious wounding.” “There’s no reason to specifically single out people with HIV,” she said.
Cedric Pulliam, co-founder of Ending Criminalization of HIV and Overincarceration in Virginia, or ECHO VA, said the group will continue to work with advocates and legislators to change the law, “whether it’s this year or the next.”
“When you’re a felon, it messes up your career, your housing, your education — your entire mental state,” said Pulliam, a public health expert at the CDC. “We want to focus on the rehabilitative things we can do rather than punish people.”Last session ECHO VA didn’t back a less comprehensive version of the bill, because it “didn’t push the needle far enough,” co-founder Deidre Johnson told NBC News. She wasn’t sure McClellan’s bill, which included repeals of the donation ban and mandatory testing, would succeed. “We knew we wouldn’t get everything but we were shocked we got what we did,” she said.
But it wasn’t a bloodless battle, Johnson said.
“It did give us some heartache to hear the draconian and outdated rhetoric around HIV” during the debate,” she said. “It was a real gut-check. We realize we have a lot more education to do. But now Virginians are talking about HIV and we’re glad it’s in a public forum.” Since gaining control of both houses in 2019, Virginia Democrats have moved swiftly to advance LGBTQ legislation: In 2020, lawmakers banned so-called conversion therapy on minorsand became the first Southern state to pass anti-discrimination protections for the LGBTQ community.
Just last week, a bill banning the use of the so-called panic defense, used to mitigate violent crimes against LGBTQ people, passed with clear majorities in both houses.
“We’ve made generational change in less than two years,” McClellan said. “I think the public was there, I think there were even Republicans that were there. But the GOP leadership wouldn’t let [LGBTQ rights legislation] out of committee.”
The bill’s passage helps to cement Virginia as a leader on LGBTQ rights. On Tuesday, the Congressional HIV/AIDS Caucus reintroduced the REPEAL Act, which provides incentives to states that reform their HIV exposure laws.
Sponsored by Reps Barbara Lee, D-Calif., and Jenniffer González Colón, R-Puerto Rico, the bill also directs the Health and Human Services and Justice departments to review policies that criminalize people living with HIV.
“We cannot achieve our shared goal of an AIDS-free generation while these laws are on the books,” Lee said in a statement. “It is past time that we repeal these harmful and discriminatory laws and instead focus our efforts on promoting public health equity and public awareness.”
President Joe Biden has indicated he supports the REPEAL Act on his policy site, saying HIV exposure laws have no basis in science and “perpetuate discrimination and stigma towards people with HIV/AIDS.”
A study that could one day lead to a potential HIV vaccine has shown promising results, scientists have said.
Researchers from the International AIDS Vaccine Initiative (IAVI) and Scripps Research say that a phase-one trial has shown “proof in principle” for a new type of vaccine that could be used against the virus.
An effective vaccine to prevent HIV infection has proved elusive for nearly four decades, not least because the virus constantly evolves into different strains to evade the immune system.
However, the trial found success in “stimulating production of rare immune cells needed to start the process of generating antibodies” that could neutralise diverse strains of HIV.
The trial succeeded in generating cell production in 97 per cent of participants, though researchers stressed it is only a first step.
Professor William Schief, executive director of vaccine design at IAVI’s Neutralizing Antibody Center, said in a release: “This study demonstrates proof of principle for a new vaccine concept for HIV, a concept that could be applied to other pathogens, as well.
“With our many collaborators on the study team, we showed that vaccines can be designed to stimulate rare immune cells with specific properties, and this targeted stimulation can be very efficient in humans.
“We believe this approach will be key to making an HIV vaccine and possibly important for making vaccines against other pathogens.”
The researchers are now partnering with biotechnology company Moderna to develop and test an mRNA-based vaccine – the same radical approach employed in the creation of coronavirus vaccines.
U.S. regulators have approved the first long-acting drug combo for HIV, monthly shots that can replace the daily pills now used to control infection with the AIDS virus.
Thursday’s approval of the two-shot combo called Cabenuva is expected to make it easier for people to stay on track with their HIV medicines and to do so with more privacy. It’s a huge change from not long ago, when patients had to take multiple pills several times a day, carefully timed around meals.
Vials of the HIV treatment Cabenuva.ViiV Healthcare via AP
“That will enhance quality of life” to need treatment just once a month, said Dr. Steven Deeks, an HIV specialist at the University of California, San Francisco, who has no ties to the drug’s makers. “People don’t want those daily reminders that they’re HIV infected.”
Cabenuva combines rilpivirine, sold as Edurant by Johnson & Johnson’s Janssen unit, and a new drug — cabotegravir, from ViiV Healthcare. They’re packaged together and given as separate shots once a month. Dosing every two months also is being tested.
The U.S. Food and Drug Administration approved Cabenuva for use in adults who have had their disease well controlled by conventional HIV medicines and who have not shown signs of viral resistance to the two drugs in Cabenuva.
The agency also approved a pill version of cabotegravir to be taken with rilpivarine for a month before switching to the shots to be sure the drugs are well tolerated.
ViiV said the shot combo would cost $5,940 for an initial, higher dose and $3,960 per month afterward. The company said that is “within the range” of what one-a-day pill combos cost now. How much a patient pays depends on insurance, income and other things.
Studies found that patients greatly preferred the shots.
“Even people who are taking one pill once a day just reported improvement in their quality of life to switch to an injection,” said Dr. Judith Currier, an HIV specialist at the University of California, Los Angeles. She consults for ViiV and wrote a commentaryaccompanying one study of the drug in the New England Journal of Medicine.
Deeks said long-acting shots also give hope of reaching groups that have a hard time sticking to treatment, including people with mental illness or substance abuse problems.
“There’s a great unmet need” that the shots may fill, he said.
Separately, ViiV plans to seek approval for cabotegravir for HIV prevention. Two recent studies found that cabotegravir shots every two months were better than daily Truvada pills for keeping uninfected people from catching the virus from an infected sex partner.