PrEP stands for Pre-exposure Prophylaxis, protection before exposure to HIV. It’s a once a day pill called Truvada for people who are HIV negative to protect them from getting HIV. PrEP was approved by the FDA in 2012, and by the U.S. Centers for Disease Control for use in HIV prevention.
I recently attended the National PrEP Summit with other HIV prevention professionals from around the country. The two-part take away for me could not have been any clearer: PrEP works, and there are so many more people who should be using it. Throughout the country, PrEP is disproportionally underutilized by women, African Americans, and Latinos. There are many challenges in getting the word out about PrEP, especially in these populations.
I have said before, if you had told us in the 1980s and 90s that there was a pill that could have prevented HIV, people would have been falling all over each other to get it. So, why not now? Although a growing number of people are beginning to use PrEP as part of their personal HIV prevention strategy, it has not taken off as quickly as one would think. There are a variety of reasons for this, the first clinical trials showed that PrEP was only 44% effective, not all that exciting. However, when they dug deeper into the data it showed to be up to 99% effective for those in the study who actually took the medicine every day as prescribed. Now we’re talking!
Many people, especially in certain populations have still not heard of PrEP, or have not heard how effective it is in preventing HIV. There has also been some stigma related to taking PrEP (similar to birth control when it first came out in the 60s). Early PrEP users were often referred to as “Truvada Whores”. Fortunately, this has begun to wane in the Gay community, where it is now being viewed as a positive thing that a potential sexual partner has been protecting themselves from HIV. Other barriers in getting people on the PrEP bandwagon include the high cost, and medical providers who are not comfortable prescribing it.
While PrEP is very expensive, $1,300 a month, it’s covered by most health plans including Medi-Cal. There are also patient assistance programs that can help with co-payments. Although many non-HIV specific doctors are not knowledgeable, and therefore uncomfortable, prescribing PrEP (or even talking to their patient about sex), we are fortunate here in Sonoma County to have several local health centers that are eager to talk to their patients about starting PrEP. California just passed a law requiring HIV test counselors to tell every person who tests negative about PrEP.
Face to Face does the majority of HIV testing in the county. We’ve been handing out PrEP brochures, and referring people to PrEP providers for quite a while. We are strong advocates for using every tool out there to end HIV transmissions in Sonoma County, and believe PrEP is our most powerful prevention tool yet. Each time we deliver the news that someone is HIV positive, I wonder if this person had heard of PrEP, considered it, thought they didn’t need it, or couldn’t afford it. A person does not need to be at high risk for getting HIV, they just have to be at risk.
The PrEP vs condoms controversy: Can’t people just use condoms? Sure, and many people do and feel comfortable with that level of protection. However, condoms don’t work at all if they’re left in the bedside drawer, just like PrEP doesn’t work if you don’t take it. Many people have a hard time (pun intended) with condoms, and therefore don’t use them regularly. Most see PrEP as an extra layer of protection and use them in conjunction with condoms. Some choose to use PrEP only, and do not use condoms. Yes, public health folks are concerned about increases in other sexually transmitted diseases. And, while there is currently a significant spike in Chlamydia, Syphilis, and Gonorrhea in California and in Sonoma County, it has not been shown that PrEP is to blame. And remember, these sexually transmitted infections are all curable, whereas there is still no cure for HIV.
So, PrEP is effective. There has been only one known case of someone contracting HIV while on PrEP, owing to a rare Truvada-resistant strain of HIV.
And, PrEP is safe. Most people experience no side effects and those who do say they are mild and last less than a month.
And, PrEP is available locally, and in most cases, affordable.
The enthusiasm and hope of ending HIV at the National PrEP Summit got me thinking about myself. I’m a single Gay man. I’m 62, and not quite as “popular” as I was in my 20’s, but couldn’t I use another layer of protection? Why not take PrEP myself? I called my doctor, got labs done to make sure I’m HIV negative, a full STD screening, checked my kidney function and bone density (all good tests I haven’t had in a long time), and now I’m ready to start my once a day pill. Who knows, maybe I’ll become more “popular” because of it, lol.
If you, or someone you know is curious about PrEP, come in and talk to one of our HIV Test Counselors. Get more information, have your questions answered, and if you’re ready, get a referral to a local provider. Test Counselors are available on a drop-in basis, Tuesday through Friday from 9:00 am to 4:30 pm at the Face to Face office at 873 Second Street, Santa Rosa.
In 2017, the patents for two antiretroviral drugs for HIV that continue to be widely used will likely expire in the United States and generic alternatives at lower market prices could be introduced. Some have long awaited this occurrence, hoping for increased competition and a drive to lower prices for all HIV medications. However, it is an open question whether generic competition, at least in the short term, will actually materialize or if it does, lead to reduced prices. If savings are realized, there is also no guarantee they will be funneled back into other critical HIV services. To explore the possibilities of wider generic availability in the United States, Project Inform co-hosted a meeting with the National Association of State and Territorial AIDS Directors (NASTAD) and the Treatment Action Group (TAG) in Washington, D.C. on September 29 and 30, 2016.
The two drugs going off patent soon are efavirenz – marketed as Sustiva – and tenofovir disoproxil fumarate (TDF) – marketed as Viread. Both efavirenz and TDF are available in combination with other antiretroviral drugs as single tablet regimens (STRs), and some of the other drugs contained in those STRs will not be going off patent. This could have significant consequences, such as the need to break up prescribed regimens into multiple pills with multiple insurance copayments.
Co-sponsors invited a diverse set of stakeholders, including providers, activists, policy makers, health economists and generic manufacturers to the meeting to ensure a broad and lively discussion. The primary segments of the discussion were:
an analysis of current drug costs across multiple payers (e.g. private insurance, Medicaid, The VA, etc.);
the potential (if any) to redirect any savings to other HIV services; and,
what the positive, neutral or negative outcomes might be for people living with HIV and front-line providers when generic HIV drugs become available.
As became clear through early discussions, the drug purchasing systems in the United States are incredibly convoluted, vary significantly by payer source, and are fairly opaque to those seeking to understand or reform purchasing systems.. Appearances can be deceiving. The price actually paid by private and public payers is almost never publicly available as negotiations are protected by privacy agreements. Because of certain purchasing mechanisms , public programs such as Medicaid or public health clinics or hospitals may be paying very little and generating program income on some older brand drugs before they go off patent. This income could significantly decrease with the introduction of generics, depending on a number of factors, including how the generics were priced and whether or not supplemental rebates were negotiated.
Examination of the generic market and payer purchasing systems raised real questions about how much money could actually be saved within a system on generic versions of HIV drugs, certainly in the near future. It is unclear where savings might be possible and how much savings would be generated by the entry of generic HIV drugs into various health care settings. Generic manufacturers and some academic studies have previously stated that significant savings could be generated but a closer examination of generic competition and health care systems made it clear that more analysis is necessary. This is not to say that generic competition is inherently bad or unuseful as a bargaining chip to lower health care costs, but that the system is so complex and everchanging that it will take considerable effort to unravel the potential outcomes of different possible scenarios.
In most cases, there are no mechanisms for savings on drug costs within most health systems to accrue back to other HIV services. Some experimental comprehensive care programs in one state are being attempted, but there is no guarantee that such programs will continue or be could be adopted in other states.
Finally, there is the fear among some advocates and providers that more aggressive cost containment measures, such as the need for a provider to get prior authorization from an insurer in order to prescribe brand name or single tablet regimens drugs, could result in some people with HIV having to take less tolerable or simple regimens and an increase in the time spent by providers and their staff dealing with the ever-changing rules and policies put in place by payers.
Though the participants agreed that the hopes once expressed about the potential for generics to usher in lower drug prices for all HIV medications in the United States are perhaps not grounded in our current reality, the activists and providers who gathered on the second day were determined to identify actions that could be taken now to ensure that benefits might be achieved. In addition, it was decided to further explore what protections might be necessary for patients and their providers to ensure access to standard of care HIV treatment in all health care systems with the entry of generic HIV drugs.
These actions have been prioritized and are being refined by the co-sponsors. They will be outlined in in more detail in recommendations put forward by the co-sponsors and we will work on implementation of some of the prioritized suggestions, which include a modelling project that would help to better understand potential cost savings and/or program income loss with the entry of generic HIV drugs. Project Inform will provide updates on these important efforts as they become available.
The ultimate impediment to a cure for HIV infection is the presence of latent, HIV-infected cells, which can reawaken and produce new virus when antiretroviral drug therapy is stopped. These latent, HIV-infected cells are untouched by antiretroviral therapy and are unseen by the immune system. Moving medicine closer to a cure for HIV, scientists at Blood Systems Research Institute (BSRI), the University of California at San Francisco (UCSF), and the University of Hawaii have discovered that the human sugar-binding protein galectin-9 potently forces latent HIV out of hiding, and poisons the virus on its way out.
Building off of their earlier studies that identified key human genes involved in maintaining the latent, hidden state of HIV-infected cells, the paper’s lead author, Dr. Mohamed Abdel-Mohsen, Scientist at BSRI and UCSF School of Medicine, and colleagues used cutting-edge technologies to demonstrate that galectin-9, a beta-galactoside-binding lectin, reactivates latent HIV and renders infected cells visible to the immune system. This concept of therapeutically forcing latent HIV out of hiding as a curative approach is known as the “shock and kill” HIV eradication strategy.
Dr. Satish Pillai, lead researcher on the study, Associate Investigator at BSRI and Associate Director of the UCSF-Gladstone Institute of Virology & Immunology Center for AIDS Research, explains, “For nearly two decades, antiretroviral therapy has demonstrated efficacy in suppressing HIV replication, but these drugs do not completely clear viral infection or fully restore health. We need a means to draw out the virus from its hidden reservoirs within the body and allow the body’s own immune system to eliminate it.”
Beyond subjecting latent HIV-infected cells to destruction by the immune system, the team found that galectin-9 strongly increases levels of an antiviral protein called “APOBEC3G” in infected cells. APOBEC3G is a lethal mutagen that destroys the genetic code of viruses including HIV. This ensures that virus that comes out of hiding at the hands of galectin-9 will be sterilized on its way out of the cell, preventing any further infection. These findings reveal that galectin-9 is a new weapon in the HIV cure arsenal, promoting eradication of the latent HIV reservoir in infected individuals on antiretroviral therapy.
The research was published in PLoS Pathogens and is an open access manuscript.
An additional revelation in the authors’ study is that galectin-9 works by manipulating sugars on the surface of HIV-infected cells to deliver the signals that force latent HIV out of hiding. “Galectin-9 binds to certain classes of sugars on the surface of cells to start a chain reaction that forces HIV out of hiding. There’s been very little attention paid to how the sugar coating on the surface of human cells affects the fate of the virus that lies inside. This sugar coating may hold the key to new therapeutics that can be harnessed to cure HIV and possibly a range of other infectious diseases.” says Abdel-Mohsen.
Pillai and Abdel-Mohsen also see the potential for galectin-9 to alter the current course of treatment for HIV, which involves life-long adherence to antiretroviral therapies to prevent latent stores of the virus in the body from reactivating and infecting new cells. “Our findings make us optimistic that future HIV treatments can eliminate all traces of the virus from the body,” says Pillai. “Ultimately, we hope that galectin-9 gets us one big step closer to a cure.” says Abdel-Mohsen.
The study was funded in large part by the amfAR Institute for HIV Cure Research and by the National Institutes of Health (NIH), with additional support from the University of California and the San Francisco-Gladstone Institute of Virology & Immunology Center for AIDS Research. The findings are among the first to be generated by researchers supported by the amfAR Institute, which was announced in December 2015. The centerpiece of amfAR’s Countdown to a Cure for AIDS initiative, the Institute brings together leading HIV researchers working collaboratively to address the scientific challenges that stand in the way of a cure.
An HIV vaccine based on how the adult immune system responds to the virus could take a long time to build protection, say researchers, who after looking at how HIV affects infants, suggest mimicking their immune response may offer a better model.
vaccine vials and hypodermic
The researchers suggest developing HIV vaccines that mimic infant immune responses may lead to faster-acting, effective protection against the virus.
In the journal Cell, researchers led by a team from the Fred Hutchinson Cancer Research Center, Seattle, WA, describe how broadly neutralizing antibodies to HIV can arise in infants within a year after infection – much more quickly than in adults.
Even though scientists have accumulated mountains of information on HIV, the prospect of a protective vaccine remains elusive. For a vaccine to be effective, it must act relatively quickly to trigger an immune response with the right mix of antibodies to eliminate the virus.
Moreover, an effective HIV immune response also adapts to the virus during the infection, and it tweaks its initial antibody response by adding antibodies that have undergone “somatic hypermutation.”
Somatic hypermutated antibodies have enhanced ability to bind to and block the pathogen and form an essential component of a broadly neutralizing response.
In the adult immune system, this process can take years – even decades – to produce an effective, broad immune response that is capable of protection against HIV.
A vaccine that mimics the adult immune response would, therefore, take too long to provide protection.
Infant antibodies to HIV produced within a year
In their study, the team examined samples taken from infants in Nairobi born to HIV-positive mothers in the years before antiretroviral drugs were developed.
They found that the infant immune system can produce broadly neutralizing antibodies against many HIV variants within a year after infection – and with less fine-tuning than previously thought.
Senior author Dr. Julie Overbaugh leads a lab at the Fred Hutchinson Cancer Research Center that investigates mechanisms of HIV transmission and disease development. She says that in contrast to studies of HIV in adults, this study enabled them to “document a case in infants where a broadly neutralizing antibody developed in a time frame and in a way that is something that we could consider mimicking with a vaccine.”
When HIV infects a human, their body cannot control the virus – “it’s too late,” explains Dr. Overbaugh. Thus, broadly neutralizing antibodies “are really a response to the replicating virus and the evolution of the virus.”
However, to be practical, an HIV vaccine needs to trigger an effective immune response within months – not years.
The new study builds on previous findings that unexpectedly found broadly neutralizing antibodies can be generated early in life.
In that study, the team used blood samples from infants who, with their mothers, took part in a breast-feeding study in the Kenya Research Program. The samples were collected before antiretrovirals were available that can protect infants from becoming HIV-infected through breast milk.
Evidence of polyclonal response
In the new study, the team took a closer look at the antibodies in the infants’ blood. They examined the antibody response of one baby in particular – the child was HIV-negative at birth but was infected by the age of 4 months.
The researchers found the infant’s blood contained evidence of what is called a “polyclonal response.”
Dr. Overbaugh explains that all adults studied so far have produced immune responses that are dominated by a single, specific antibody. Polyclonal responses are much harder for viruses to elude and much more likely to protect against a wider range of variants.
The team also found that broadly neutralizing antibodies in the infant samples had gained their HIV-blocking abilities without exhaustive rounds of somatic hypermutation, which – in theory – shortens the time it takes to produce a broadly neutralizing response.
In another part of the study, the team found that the infant broadly neutralizing antibodies target a different site on HIV to that targeted by adult antibodies – again suggesting a different path from infection to protection.
Infants’ broadly neutralizing antibodies could lead to HIV vaccine
These results suggest broadly neutralizing antibodies from infants could lead to a fast-acting, effective HIV vaccine. However, the roadmap still needs to be charted, and many questions remain.
For example, do infant antibodies differ because of differences in the types of HIV variants they are exposed to, or because of unique features in the infant immune system?
Dr. Overbaugh suggests perhaps infants are exposed to a different spectrum of HIV variants than adults because those viruses have already been exposed to their mothers’ immune systems, so the ones that pass into breast milk are shaped by the mothers’ antibodies.
However, if it turns out that infant immune systems have a unique ability to make broadly neutralizing antibodies against HIV quickly, then perhaps vaccinating babies is the way to early protection.
The researchers are already doing further research to confirm their findings in blood samples taken from another baby whose HIV variants have led to many studies of the structure of the virus.
They are also taking a closer look at the process of HIV antibody fine-tuning, and hope to deploy any new findings into developing preclinical models of infection that may also produce fast, protective responses.
A new study funded by amfAR, The Foundation for AIDS Research conducted by researchers at the San Francisco VA Medical Center (SFVAMC) observes that pharmacological enhancement of the immune systems of HIV patients could help eliminate infected cells, providing an important step in the ongoing quest to find a lasting HIV cure.
The study, titled “Stimulating the RIG-I Pathway to Kill Cells in the Latent HIV Reservoir Following Viral Reactivation,” addresses the persistence of latent HIV reservoirs in patients who are on antiretroviral therapy. Latent HIV reservoirs are established during the earliest stage of HIV infection, and they are infected with HIV even though they are not actively producing the virus. Although antiretroviral therapy can reduce the level of HIV in the blood to an undetectable level, latent reservoirs of HIV continue to survive. When a latently infected cell is reactivated, the cell begins to produce HIV again. For this reason, antiretroviral therapy cannot cure HIV infection.
According to the study, HIV latency depends on immune system suppression, including immune system responses that detect viral pathogens and induce the destruction of infected cells. The study shows that retinoic acid can stimulate the innate immune system into eliminating HIV-infected cells. In particular, acitretin, an FDA-approved retinoic acid derivative, can increase HIV transcription in the latent HIV reservoir and allow the innate immune system to target and destroy HIV infected cells.
“The current model of HIV treatment can help manage symptoms and increase the quality of life for patients, but it is not a cure,” says the study’s lead author Peilin Li, MD, MHS, Research Associate at SFVAMC, and an Assistant Adjunct Professor at the University of California, San Francisco School of Medicine. “HIV patients on antiretroviral medications must take them for the rest of their lives, and they often experience adverse side effects.”
“It is important to strengthen the body’s defense system against the virus. This will help the antiretroviral drugs do their job,” says Dr. Li. “We want the immune system to recognize and kill the virus. By boosting immune response, the body will be able to kill cells in the latent HIV reservoir that are still capable of producing HIV.”
Dr. Li is hopeful that the study’s findings will lead to new ways of thinking about treating HIV. “I think this can open new doors to fighting HIV. With further research, we can create clinical solutions that can boost immune system functioning and find a lasting cure for this disease. This is a patient-centered approach to HIV treatment that moves beyond treating symptoms and toward whole health.”
This study was published in Nature Medicine magazine on June 13, 2016. You can read the study at: http://go.nature.com/1ro7w9j
The Centers for Disease Control recently published a new brochure explaining how individuals—through a variety of insurance and medication assistance programs—can cover the cost of PrEP.
The brochure includes links to a community health center location tool, PrEP assistance programs, and co-pay programs, and gives a breakdown of the steps to take in order to pay for the medication, lab tests, and clinic visits. Download the brochure, here.
Rectal microbicide gels, applied either daily or before and after sex, are currently being investigated as an option for HIV pre-exposure prophylaxis (PrEP). Given that many people who have anal sex already use lube, one hope is for an HIV-prevention product that people could essentially use in place of a lube. But can gels provide enough coverage across rectal tissue if people don’t use an applicator?
Studies of rectal tenofovir microbicide gels, such as the MTN-017 study, provide rectal-specific applicators for people to use to insert the gel. Although applicators deliver a precise dose, they may challenge product acceptability by being bulky, inconvenient and unappealing to users.
“Use of applicators does not mimic real world lubricant use during sex,” explained Eugenie Shieh, MD, from The Johns Hopkins Hospital.
If a rectal microbicide gel is approved for HIV PrEP, finding an effective application that works in the lives of potential users will be crucial to its success.
At CROI 2016, Shieh presented results from a study investigating whether a gel, applied by men in the way they would normally apply lube, could deliver a similar volume, in the same areas of the colon, as gel delivered by an applicator. Five men with a history of receptive anal intercourse used a radiolabeled gel that could later be detected on a SPECT/CT body scan.
Participants tested three different deliveries: gel via applicator (3.5 or 10 mL) and a radiolabeled lube (up to 10 mL) that they were told to apply as they normally would before sex. After applying the lube, participants were asked to “simulate anal intercourse” with an artificial phallus (which would effectively push the lube into the colon).
Although this was a small study, her team found that manual dosing delivered a smaller amount of gel that was retained in the colon, with more variability between users. About 3% of the gel was retained inside the colon after manual gel use. This is compared to 95% of gel retained in the colon with a 10 mL dose delivered by applicator, and 88% of gel retained with a 3.5 mL applicator dose.
“For manual dosing, the dose retained was 32-fold less than the 10 mL applicator dosing,” explained Shieh.
Detection of radiolabeled gel on SPECT/CT scan with manual gel application. Slide: Eugenie Shieh, MD
The researchers also measured how far the gel distributed along the colon by looking at the SPECT/CT scan images and using a computer algorithm to estimate concentrations of the gel. Shieh reported that the manual and applicator distributions were similar, but that manual dosing was associated with less consistent distribution of gel across the colon.
Shieh concluded that rectal microbicides applied as a lube “may not provide adequate drug concentrations or reliable mucosal coverage where needed,” and that, “lube dosing may require a different formulation than applicator dosing.” Increasing the concentration of the drug contained in the microbicide lube, from 1% (the percentage of tenofovir currently being tested as a rectal microbicide) to 10% may help, said Shieh, but that “ultimately, the feasibility of manual dosing will vary with each rectal microbicide.”
The potent protection from HIV afforded by Truvada as PrEP allows men to have sex with less worry and fear of HIV. But some worry that the inclusion of PrEP as a public health strategy will lead people to abandon condoms—which still have a role to play in further reducing risk of HIV and other STIs. In San Francisco—even before PrEP’s availability in 2012—rates of STIs among men who have sex with men have been steadily increasing and rates of condom use have gone down.
BETA wanted to know—what do PrEP providers think? How do these practitioners, who see clients every three months for sexual health screenings and STI testing, talk to their clients about condom use, STIs and navigating the complicated landscape of protected, or safer, sex?
To find out, BETA talked to Stefan Rowniak, MSN, PhD, a PrEP provider and nurse practitioner at San Francisco City Clinic and researcher and assistant professor at University of San Francisco; Pierre-Cédric Crouch, PhD, ANP-BC, the nursing director at the San Francisco AIDS Foundation health and wellness center Strut; Robert Blue, a PrEP program coordinator for San Francisco City Clinic; and Hyman Scott, MD, who leads the Ward 86 PrEP Clinic at San Francisco General Hospital.
Here’s what they said.
The rates of gonorrhea, chlamydia and early syphilis infection have been on the rise in recent years in San Francisco. Do you see this as a major problem?
Pierre-Cédric Crouch, PhD, ANP-BC
Pierre-Cédric Crouch, PhD, ANP-BC: Obviously nobody wants to get gonorrhea, chlamydia, or syphilis, but these are risks that we have from living. The only way to completely avoid them is to not have sex at all and that’s not who we are as humans. You can also get the flu from having sex, or strep throat. People die from the flu. People don’t die from gonorrhea, but there’s more stigma attached to gonorrhea than the flu. The levels of STIs are going up in San Francisco—and have been since before PrEP was available here—but they’re nowhere close to what they were in the 70s and 80s.
Stefan Rowniak, MSN, PhD
Stefan Rowniak, MSN, PhD: That’s a very difficult question—but one the community is going to have to answer. If people suddenly find themselves saying, ‘My god, this is the third time I’ve gotten gonorrhea in three months,’ they may think, ‘What can we do about this?’ It’s going to take people realizing that they don’t want to get gonorrhea over and over again every time they have a new sex partner. Health providers will be there to help the discussion along—but we’re not the sex police. We are there to inform and help people make those decisions themselves.
Since gonorrhea, chlamydia and syphilis can all be treated, how do you talk to clients about the potential harms associated with these STIs?
Hyman Scott, MD
Hyman Scott, MD: At this time, these STIs are all treatable with antibiotics, but just because they are treatable do not mean that they are benign. What is a concern is that we are seeing rising rates of drug-resistant gonorrhea, and we shouldn’t forget that gonorrhea can cause sterility. And while syphilis is still treatable with penicillin, with the increase in total cases, we’re seeing more of the complications that come along with syphilis such as neurosyphilis, vision impairment, and vision loss. Giving people the full picture is important—not to spread fear, because we want to have a sex-positive approach when we’re talking about sex—but so that people have the information they need to make decisions about their sexual health.
Some people worry that PrEP is, or will, cause people to abandon condoms. Are your clients changing their condom use now that they’re on PrEP?
Robert Blue
Robert Blue: Yes and no. There are some people who start taking PrEP and they actually start thinking more about their sexual health. Their thought seems to be, ‘Well, I’m taking PrEP for my sexual health, why would I then go out and not use condoms?’ There are people who didn’t use condoms before PrEP, and that doesn’t change. And there are some people who, once they started taking PrEP decided to stop using condoms.
Crouch: We haven’t seen much change, but it’s difficult to measure. Some people will come in and report that they used condoms all the time before they started PrEP. But when you ask a few more questions, you find out that there were exemptions to it—the person didn’t use condoms with their main partner or those few times with their fuck buddy. So it wasn’t really 100% condom use to begin with.
Scott: I think for some clients, there is a change in the way that they decide to use condoms [on PrEP], but there’s a lot of variability. Some people may change their condom use with certain partners, but not others. With the rise in STIs and increased uptake of PrEP, there is a real desire of some to make that linkage and say that one is causal to the other. We have seen a rise in STIs before the increased uptake of PrEP. Studies that have systematically looked at this haven’t found much of an overall change in the level of condom use among PrEP users, but it will also be important to monitor as PrEP roll-out expands in more real-world settings. Anecdotally, we’ve had people who don’t change their condom use at all. It’s definitely something we need to keep track of, but at this point we don’t have data to say that initiating PrEP is the reason people change their condom use, if they change it.
Do condoms still have a role to play in gay men’s sexual health alongside PrEP?
Crouch: Condoms still have value. They do a good job of reducing transmission of gonorrhea and chlamydia—less so for syphilis. They don’t provide 100% protection, but they do have value. All in all, we don’t know five years from know how people will use condoms when they’re on PrEP. I could see it being similar to what happened for oral sex—in the 90s, when people thought you could get HIV from oral sex, there was a big push for people to use condoms for oral sex. I don’t know if that’s what people really did, but now that we know the risk of HIV transmission from oral sex is so rare, I think people in general gave up on feeling like they should use condoms for oral sex. Of course there’s still a risk of getting or transmitting other STIs but the risk of HIV is so slight with oral sex. It’s the same way for anal sex if you’re on PrEP.
Rowniak: I don’t believe people will completely abandon condoms in favor of PrEP. Rather, I think people will use condoms with some partners and in some instances and not in others. I think people feel, to a certain extent, a little frightened after spending years and years using condoms, and all of a sudden not using them at all. So the pendulum might swing back and forth until it reaches a place to settle.
Blue: We know that while PrEP is highly effective in preventing HIV transmission, it is not 100%. Many people still feel more comfortable using condoms while taking PrEP. We also know that PrEP doesn’t prevent the transmission of other STIs and that condoms can be an effective STI-prevention strategy.
Scott: Condoms absolutely have a role to play. One thing to remember is that we’ve never studied PrEP versus condoms—PrEP has always been inclusive of condoms. The package that includes PrEP is not just one pill per day. It’s about condom promotion, too. There are a variety of ways that people can have protected or safer sex, and we want to give people the tools that fit within their sex lives and support them with all of these options.
Do you advise your clients to use condoms? And if so, how do you have those conversations?
Blue: Yes, we do. Ultimately, we want people to think logically or rationally about their sex lives (acknowledging that sex is not often our most rational form of self-expression!). We want people to be able to evaluate their risk of HIV and STIs and decide on what prevention strategies make sense for them.
Rowniak: I make a point to talk with clients about when it might be appropriate to use condoms—and when it might make sense to reintroduce condoms back into sex. These conversations help get people to think about using condoms, and that’s really the first step. Introducing this new thought about condoms helps people think about ways they might like to be a little more circumspect.
Crouch: Our job is to provide education and have the client come up with their own informed sexual health plan. We tell clients that PrEP isn’t 100% effective at preventing HIV infection, even though we haven’t had any infections on PrEP yet—because nothing in life is 100%. Condoms provide extra protection against gonorrhea and chlamydia. We frame it as, ‘Using condoms with PrEP is your best overall protection.’ But we don’t lecture anyone to do, or not do, anything. We’re here to inform and help support people in whatever they decide to do. If condoms haven’t been a problem for a client, they should definitely continue to use them—though condoms aren’t always easy for people to use. They can break. Some people tell us they have trouble maintaining an erection with them. Some say condoms reduce intimacy in relationships. It’s ultimately an individual decision. There is no right or wrong answer.
Scott: I’m humble enough to know that I only get the opportunity to spend 30 minutes, maybe an hour, talking with patients about a variety of medical conditions including their sexual health, which is balanced with all the other needs and considerations in their daily lives. I give them guidance and recommendations but I don’t try to convince them to use condoms if they’ve already made up their mind about condom use. I meet my patients where they’re at and see how open they are to exploring condom use. Recently, I saw someone who was diagnosed with early syphilis. We started treatment [for syphilis] but then also talked about why he didn’t use a condom with this new partner, despite his ‘rule’ to use condoms with new partners. His response that, ‘The guy was just my type’ was incredibly insightful and understandable. So there was something powerful about desire and passion, and wanting to make a connection with his partner that influenced his decision making. So I explore the barriers and facilitators people may have for condom use, but never pass judgment on their decision.
For more information about PrEP services at the gay men’s health and wellness center in the Castro, Strut, visit www.strutsf.org. Find out more about the Ward 86 PrEP Clinic at San Francisco General Hospital. Continue learning more about PrEP at www.prepfacts.org or on BETA.
Let’s face it. Adulting is hard. But much more important than overcoming the Sunday Scaries and using Excel to keep track of just how bad you are at actually sticking to a budget is your health. There’s a good chance you’ve heard of PrEP, but how much do you really know about it? PrEP (pronounced “prep” and commercially known as Truvada) is an abbreviation for pre-exposure prophylaxis and it is an anti-viral treatment approved by the FDA in 2012 that your physician can prescribe to you in daily doses as a method of preventing new HIV infections.
Many people, with good reason, have lauded the development of this treatment as a modern miracle. So we should all be on it, right? Not so fast. From a public policy perspective, it makes a lot of sense to recommend the use of this drug to the masses. After all, HIV-AIDs is a terrible epidemic and there are positive network effects when entire populations become immune or resistant to infections, as with vaccines. But at a personal level, the decision to start PrEP is a bit more complicated. Let’s look at some of the key considerations, questions and implications.
Are there side effects?
PrEP has several known side effects to consider. Some, like headaches, nausea and problems sleeping are minor and tend to wear off. However, there are some potentially life-threatening complications including increased lactic acid in the blood, liver damage, kidney failure and decrease in bone density. In order to guard from all of these, it is mandatory for patients on PrEP to see a physician at least once every 3 months for a full panel of blood tests, according to Truvada.com.
Is PrEP common?
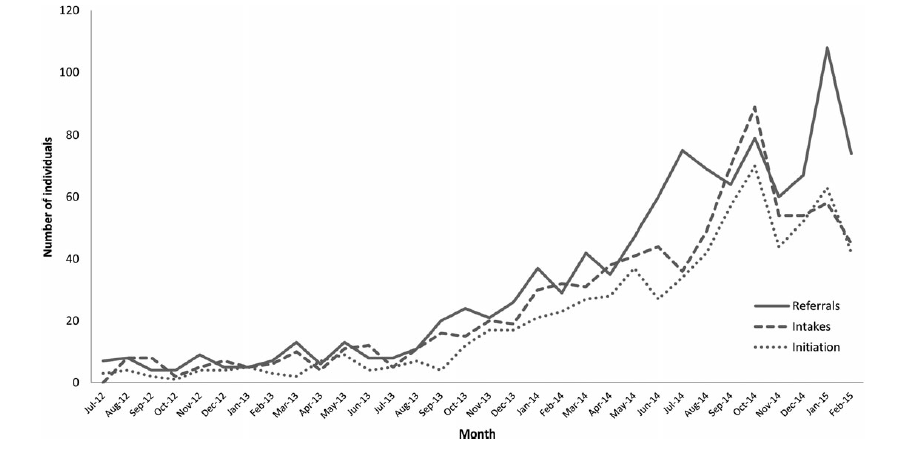
Increasingly so. Anecdotally, I can tell you that I see men on dating and hookup apps advertising their use of PrEP more and more. I also hear friends talk about it and admit to taking it on a fairly regular basis. It’s understandable that there may be some negative stigma associated with a gay man who chooses to take PrEP — it implies some level of promiscuity — but the community has gotten past that issue quickly, due to its important role in public health. In the way of more hard evidence, the following graph shows patient interest in PrEP at Kaiser Permanente San Francisco; it illustrates the same increased use.
Does it protect from other STIs?
No. This is actually a really interesting point to stop and look at a few recently published STI incidence statistics and consider their relation to the increasingly common use of PrEP amongst gay men. A few months ago, the Center for Disease Control (CDC) released its annual report on the incidence of several STIs. In 2014, there were increases in the percent of the general population diagnosed with chlamydia, gonorrhea and syphilis for the first time since 2006. As usual, women and people aged 15-24 are at higher risk than other cohorts, but there are some startling trends in the gay male population over the past few years too.
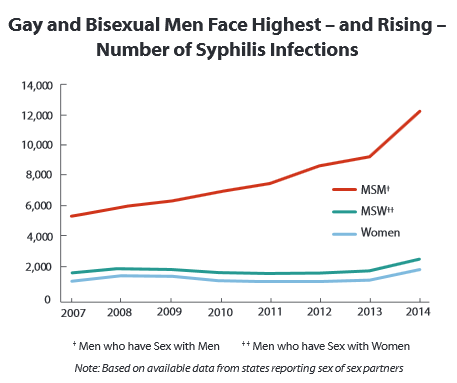
The graph below, also from the CDC, shows that the rate of syphilis infection amongst gay men is growing much more rapidly than it is in the general population. Add to that the fact that of all men with cases of syphilis, 83 percent of them are gay and you begin to better understand a dangerous unintended consequence of a drug that prevents new HIV infections — many patients on PrEP are having unprotected sex. This is not just an assumption based on the trends. According to Kaiser Permanente, mentioned above, 45 percent of surveyed patients on PrEP reported that they were having more unprotected sex.
Cast in a less alarmist light, consider that all 3 — chlamydia, gonorrhea and syphilis — are bacterial infections that can be cured with antibiotics. So does it really matter if the use of PrEP is positively correlated to rising rates of STIs other than HIV? I mean, they’re curable. It matters. And that’s simply because not all STIs are curable, including herpes, HPV and hepatitis — the latter two of which can be life-threatening. It’s also worth noting that the same CDC report showed that, of the gay men who were diagnosed with syphilis, 51 percent also were infected with HIV. This type of co-infection is common, given that those men were likely engaged in unprotected sex and syphilis can cause open sores, which are more likely to be infected by HIV.
Is there an alternative to PrEP?
Yep, there is. Before there was PrEP, there was PEP, which stands for post-exposure prophylaxis. This treatment is often used for healthcare officials who work with HIV-infected patients and their bodily fluids in case of emergency. It’s also nicknamed “the morning-after pill for HIV.” It is an antiviral regimen, just like PrEP, except that is has to be started within 3 days of the exposure and lasts one month. The same side effects are a concern with PEP, but because the treatment only lasts one month, there is less concern about long-term issues.
So should I be on PrEP?
I don’t have an answer on this one. It is a very personal choice that you should discuss with your physician. The decision I made for myself may not be the right one for you. To get started, consider the information above and ask yourself a few questions. Do you practice unprotected sex and, if so, how often? Are you in a committed relationship? Would you prefer to have peace of mind no matter what? Will taking PrEP change your sexual behavior and are you ok with the potential consequences?
Nate Warden is a regular contributor to The Huffington Post Gay Voices blog and founder of www.ComingOut.Space, an online library of diverse coming out stories.
When HIV infects the body, it establishes a key foothold in lymphoid tissue and can persist there, despite potent therapy. But HIV is not dormant in this viral reservoir; the virus continues to replicate, move between tissue compartments and evolve – even when it is undetectable in the blood.
HIV continues to replenish its viral reservoir in lymphoid tissue even when it can no longer be detected in the bloodstream.
This was the conclusion of a new international study – led by Northwestern University in Chicago, IL, and published in Nature – that provides an important new perspective on how HIV stubbornly persists in the body, despite powerful antiretroviral therapy.
Senior and corresponding author Steven Wolinsky, a professor in medicine and chief of infectious diseases at Northwestern’s Feinberg School of Medicine, says:
“We now have a path to a cure. The challenge is to deliver drugs at clinically effective concentrations to where the virus continues to replicate within the patient.”
The HIV (human immunodeficiency virus) weakens the immune system by destroying important white blood cells, called CD4 or T cells, that fight disease and infection.
As the HIV infection worsens, the immune system gets weaker and weaker and the person becomes more prone to opportunistic infection. Acquired immune deficiency syndrome (AIDS) is the final stage of HIV infection, when the body can no longer fight life-threatening infections.
There is no effective cure for HIV, although the availability of potent antiretroviral therapies means what was once a fatal diagnosis can now be managed as a chronic disease.
The Centers for Disease Control and Prevention (CDC) estimate there are over 1,218,400 Americans aged 13 years and older living with HIV, including 156,300 (12.8%) who are unaware they are infected with the virus.
Nowadays, combinations of powerful antiretroviral drugs can reduce HIV to undetectable levels in the bloodstream of most patients. But the virus can persist in pockets in lymphoid tissue in the body and quickly appears again in the blood when patients stop taking the drugs.
This suggests the virus persists in this reservoir because it either continues to replicate at low levels, it is able to survive in long-lived infected cells – or both.
As nobody had detected viruses with new mutations, and because patients on antiretrovirals do not develop drug resistance when the virus is gone from the bloodstream, it was thought the viral reservoir only contain long-lived HIV-infected cells in a dormant state – and no newly infected cells.
For their study, Prof. Wolinsky and colleagues sequenced viral DNA from infected cells sampled from the lymph nodes and the bloodstream of three HIV-infected patients before and during their first 6 months on antiretroviral therapy.
The results showed that the virus evolved over time – and was therefore replicating – but the mutations did not indicate it was developing drug resistance.
The team then developed a mathematical model to investigate how the virus might evolve during therapy without developing drug resistance.
The model showed that drug-sensitive HIV strains tend to dominate over drug-resistant strains in the presence of low drug concentrations. But the model also showed that as drug concentration rises, this changes and the drug-resistant strains begin to dominate. And at high concentrations, HIV cannot grow at all.
This finding highlights the importance of delivering effective antiretroviral drug concentrations into the lymphoid tissue compartments, note the authors.
Antiretrovirals that penetrate the lymphoid tissue compartments where HIV can persist and replicate will be a prerequisite to the elimination of the viral reservoir and, ultimately, a step toward a cure, they suggest.
Coauthor Angela McLean, professor of mathematical biology at the University of Oxford in the UK, who led the mathematical modeling, concludes:
“The study is exciting because it really changes how we think about what is happening in treated patients. It helps explain why some strategies that tried to clear the reservoir have failed.”
In November 2015, Medical News Today learned of another study that found effectiveness of HIV antiretroviral treatment in adults may be hampered by low levels of vitamin D. That research found that patients with sufficient levels of vitamin D recovered more of their immune function during therapy than patients with vitamin D deficiency.
Written by Catharine Paddock PhD